Vertical differentiation Oligopolistic pricing models
In conditions of horizontal differentiation, the buyer's choice is determined by commitment to a particular brand,...
Slide 1
Slide 2
 Who is a neonatologist? A neonatologist is a pediatrician, just like a pediatrician, who monitors and treats children at a very early age, usually in the first year of life. The follow-up service was formed to provide assistance to children with perinatal pathology and monitor them during the recovery period. The doctor of the follow-up office focuses mainly on children under 1 year of age: premature, low birth weight, those who have undergone resuscitation and intensive care, children with various developmental disabilities. If necessary, observation continues for up to three years or more.
Who is a neonatologist? A neonatologist is a pediatrician, just like a pediatrician, who monitors and treats children at a very early age, usually in the first year of life. The follow-up service was formed to provide assistance to children with perinatal pathology and monitor them during the recovery period. The doctor of the follow-up office focuses mainly on children under 1 year of age: premature, low birth weight, those who have undergone resuscitation and intensive care, children with various developmental disabilities. If necessary, observation continues for up to three years or more.
Slide 3
 Consultation with a neonatologist A consultation with a neonatologist will help answer all your questions that young mothers may have quite often. How to bathe children correctly, how to dress a baby, how much time to spend with him in the fresh air? During a consultation with a neonatologist, the doctor will help you choose a milk formula when breastfeeding is not possible. Also, a specialist doctor will give the necessary recommendations for massage and gymnastics, and draw up an individual vaccination schedule for the child.
Consultation with a neonatologist A consultation with a neonatologist will help answer all your questions that young mothers may have quite often. How to bathe children correctly, how to dress a baby, how much time to spend with him in the fresh air? During a consultation with a neonatologist, the doctor will help you choose a milk formula when breastfeeding is not possible. Also, a specialist doctor will give the necessary recommendations for massage and gymnastics, and draw up an individual vaccination schedule for the child.
Slide 4
 When do you contact a neonatologist? If the child has the following pathology: -Prematurity; -Respiratory disorders; - Posthypoxic lesions of the central nervous system and other organs; - Intrauterine malnutrition and IUGR; -Congenital malformations; - Hereditary metabolic disorders; -Hyperbilirubinemia; -GBN; -IUI, early neonatal infection; -Blood diseases; -Other causes of postnatal adaptation disorders.
When do you contact a neonatologist? If the child has the following pathology: -Prematurity; -Respiratory disorders; - Posthypoxic lesions of the central nervous system and other organs; - Intrauterine malnutrition and IUGR; -Congenital malformations; - Hereditary metabolic disorders; -Hyperbilirubinemia; -GBN; -IUI, early neonatal infection; -Blood diseases; -Other causes of postnatal adaptation disorders.
Slide 5
 What happens at a neonatologist's appointment? 1. The doctor will ask the mother about her diet and lifestyle, examine the child, evaluate his appearance, symptoms, and behavior. 2.Measure the child’s height, weight and head circumference, listen to his heart through a stethoscope, examine the abdomen, and check his hearing and vision. 3. Advise which specialist needs to show the baby, at what age it is optimal to conduct a course of massage and gymnastics; will give recommendations for hardening. 4. She will answer questions about how to properly bathe and dress the baby, how long to walk, and help you choose a milk formula if breastfeeding is not possible. 5. Prescribe the necessary examination and treatment.
What happens at a neonatologist's appointment? 1. The doctor will ask the mother about her diet and lifestyle, examine the child, evaluate his appearance, symptoms, and behavior. 2.Measure the child’s height, weight and head circumference, listen to his heart through a stethoscope, examine the abdomen, and check his hearing and vision. 3. Advise which specialist needs to show the baby, at what age it is optimal to conduct a course of massage and gymnastics; will give recommendations for hardening. 4. She will answer questions about how to properly bathe and dress the baby, how long to walk, and help you choose a milk formula if breastfeeding is not possible. 5. Prescribe the necessary examination and treatment.
Slide 6
 What additional examinations can a neonatologist prescribe? 1. General blood test. 2. General urine analysis. 3. Stool analysis. 4. Neurosonogram (ultrasound of the brain). 5.ECG. 6. Ultrasound of the hip joints. 7.Consultations with relevant specialists.
What additional examinations can a neonatologist prescribe? 1. General blood test. 2. General urine analysis. 3. Stool analysis. 4. Neurosonogram (ultrasound of the brain). 5.ECG. 6. Ultrasound of the hip joints. 7.Consultations with relevant specialists.
Slide 7
 Half an hour is allotted for examining one patient. After examining the child, the mother is given a detailed statement with a diagnosis and recommendations for further examination and treatment, which she has the right to transfer to the local pediatrician at the clinic at her place of residence.
Half an hour is allotted for examining one patient. After examining the child, the mother is given a detailed statement with a diagnosis and recommendations for further examination and treatment, which she has the right to transfer to the local pediatrician at the clinic at her place of residence.
Pathology of premature babies. Newborns at risk. Completed by Pavlidi Christina ml-504 Teacher Petruk N.I. RUDN Moscow 2012 Full-term - a newborn baby of gestational age 38 - 41 weeks. As a rule, such a child is functionally mature and capable of living in extrauterine conditions. A premature baby is considered to be one who was born between the 22nd and 37th weeks of development with obvious signs of life. CAUSES OF MISTARRIAGE. Disorder of the maternal endocrine function (dysfunction of the ovaries, adrenal glands, thyroid and pancreas). Congenital malformations of the uterus. Previous abortions. Multiple pregnancy. Extragenital and gynecological diseases. Bad habits of the mother (smoking, alcohol, drugs, etc.) Immunological conflicts. Physical and mental trauma. Genital infantilism. CLINICAL CHARACTERISTICS OF A PREMATURE BABY. The posture of a premature baby resembles that of a fetus. Body weight 2500 g or less. Length 45 cm or less. Og and Ogre are less than the corresponding indicators of full-term children. The skin is wrinkled, dark red in color, the subcutaneous fat layer is not expressed. The bones of the arch are soft, the fontanelles and sutures are open. Ossification nuclei of the femoral head are not detected. Genital organs: in boys, the testicles are not lowered into the scrotum; in girls, the labia majora do not cover the labia minora and clitoris. Functional immaturity of organs and systems. THE DIFFERENCE BETWEEN A FULL-TERM AND PREMATURE BABY. Internal organs and systems are immature. In premature and “low birth weight” children, the body’s defenses are weaker and more imperfect. The period of adaptation to the outside world is more intense for them than for full-term babies. In this regard, adverse effects are particularly acute for children. Pathology often develops against this background. Diseases that do not pose a danger to other children are more severe in premature and “low birth weight” children. During childbirth, even without complications, the baby’s brain experiences great stress. The pressure on the membranes can be so strong that circulatory problems develop, which can lead to hemorrhages in the brain. In premature babies, brain immaturity is often accompanied by hypoxia, traumatic birth, and a lack of hematopoietic vitamin K, which also often leads to cerebral hemorrhages and strokes. Impaired cerebral circulation can lead to damage to brain structures. Against this background, the formation of cerebral palsy is possible. With mild hemorrhages, the walls of small vessels “burst” and this can lead to increased intracranial pressure. Intracranial pressure increases due to excess fluid formation in the ventricles of the brain, which presses on surrounding tissue. With minor hemorrhages, the condition in most cases is quickly compensated, the outflow of fluid from the ventricles is normalized, and the hemorrhages resolve without a trace. Severe hemorrhages, when large vessels “rupture” and blood fills all the cerebral ventricles, cause much more serious consequences, leading to: hydrocephalus, convulsions, developmental delays, and motor disorders. Such children need constant help from a neonatologist, neurologist and other specialists, in particular monitoring from the neurosensory organs (hearing and vision), since these areas of the brain can be damaged. As is known, the formation of brain structures occurs at an early stage of intrauterine development. A premature baby is born with formed parts of the nervous system, but the nervous system is immature and is often unable to properly regulate all organs and systems. It takes time. In the first days, the baby does not know how to suck independently, because the nerve impulse is not transmitted correctly to the muscles that are involved in sucking. The child is fed through a tube for a long time until the sucking reflex is formed. Very often, such children, having already learned to suck, swallow poorly. Children who have been tube-fed for a long time and have been on artificial ventilation for a long time usually begin to speak late and pronounce sounds incorrectly because the reflexes that regulate the tone of the muscles involved in the pronunciation of sounds take a very long time to form. Therefore, almost all very premature babies require the help of a speech therapist. Moreover, speech therapy classes are necessary even before the child begins to speak, in order to normalize the tone of the tongue muscles and form the correct development of speech muscles. An orthopedic surgeon examines all newborns at least 4 times (at the ages of 1, 3, 6 and 13 months). Such control makes it possible to timely detect a pathology that is often found in premature babies, such as dysplasia (underdevelopment) of joints. In children with damage to the nervous system, motor activity and muscle tone are reduced, and reflexes are weakly expressed. On the contrary, there may be excitement. Convulsive syndrome often occurs in premature infants. Brain ultrasound (brain ultrasound) is widely used to diagnose neurological disorders in children. If a child has risk factors for severe pathology of the central nervous system, he needs active treatment and follow-up by a neurologist. In premature babies, the respiratory system is also immature. There is insufficient development of lung tissue and its blood supply. More often, premature babies develop anemia and rickets. everyone. Children are susceptible to infectious diseases, often suffer from colds, otitis media, etc. Anemia is one of the most common pathologies in young children. About 20% of full-term babies suffer from this disease, and among premature babies, almost all of them develop anemia in the first year of life. The severity of anemia is higher, the lower the gestational age of the baby. In the first months of life in premature infants with very low birth weight (less than 1500 g) and a gestational age of less than 30 weeks. Severe anemia requiring red blood cell transfusion is up to 90%. All premature babies undergo audiological screening, as there is an increased risk of hearing impairment due to damage to the nervous system. Also, all premature babies are required to be examined by an ophthalmologist. The first examination is carried out at the age of 4-6 weeks, and then once every three months. Observation by an ophthalmologist is necessary to identify retinopathy of prematurity. Retinopathy of prematurity is a disease of the eyes of premature babies, often leading to irreversible loss of visual function. The main manifestation of retinopathy of prematurity is the stopping of the normal formation of blood vessels, their growth directly into the eye into the vitreous body. The growth of vascular tissue and, subsequently, young connective tissue causes tension and retinal detachment. NEWBORN RISK GROUPS Risk group 1. For pathology of the central nervous system Risk group 2. For the occurrence of purulent-inflammatory diseases Risk group 3. For anemia Risk group 4-5. For chronic nutritional disorders (hypotrophy, paratrophy) Risk group 6. For rickets Risk group 7. For the formation of malformations of the tissues of temporary and permanent teeth, caries and malocclusions Risk group 8. For thymus gland enlargement syndrome Risk group 9. For sudden death syndrome (VNS) Risk group 10. Children with manifestations of exudative-catarrhal diathesis. Risk group 11. Children with manifestations of lymphatic-hypoplastic diathesis. Risk group 12. Children with manifestations of neuro-arthritic diathesis. Risk group 13. Children from socially disadvantaged families** Risk group 1. For pathology of the central nervous system Frequency of examinations by specialists: Pediatrician for 1 year every month. Neurologist according to indications. Children II B gr. health - pediatrician monthly, neurologist at 1,3,6 months. According to indications - ophthalmologist, endocrinologist, geneticist, speech therapist, psychologist. Particular attention is paid to: Posture and position, muscle tone, reflexes, reaction to sound and light, sucking activity, the presence and nature of regurgitation and vomiting, stigmata of dysembryogenesis, size and shape of the skull, size and condition of sutures and fontanelles, sleep disturbance, "anxious "pathological neurological symptoms, weight gain, rate of neuropsychic development. Additional research methods: If necessary, neurosonography, radiography of the skull in 2* projections, ECG, biochemical blood test for calcium, phosphorus, alkaline phosphatase. Risk group 1. For pathology of the central nervous system. Main ways of recovery: Protective regime and maximum stay in the fresh air, correct hygienic care. For the syndrome of increased neuro-reflex excitability - free feeding, refusal of force feeding. In the first month, feed at least 7 times a day. Psychotherapy for a nursing woman, adherence to feeding techniques; first complementary feeding in the form of milk porridge (in the absence of paratrophy). Therapeutic massage, gymnastics, water procedures. Persistent activities on the upbringing and development of the child. Drug therapy (phenobarbital, etc.) and herbal medicine (herbal infusions: horsetail, mint, motherwort, valerian) - according to indications. Permission for vaccinations by commission: pediatrician, head. department, neurologist. If there is no pathology of the central nervous system within 6 months, the child is transferred to 1 gram. health. Risk group 2. For the occurrence of purulent-inflammatory diseases Frequency of examinations by specialists: Pediatrician for the first 7 days daily, then at 14, 21 days and at 1 month. According to indications (localized purulent infection) - surgeon, ENT doctor. Particular attention is paid to: General condition, body temperature, sucking activity, the presence of regurgitation and vomiting: weight gain. Condition of the skin and mucous membranes, umbilical wound, umbilical vessels, condition of lymph nodes, liver, spleen and other internal organs; character of stool and urination. Neurological status, hemorrhagic symptoms. Additional research methods: An. blood at 1, 3, 6, 12 months. and during acute intercurrent illnesses. An. urine at 3, 12 months. and during intercurrent illnesses. According to indications - urine according to Nechiporenko, for bacteriuria, feces for coprogram, microlandscape, culture from the throat and nose. Risk group 2. For the occurrence of purulent-inflammatory diseases The main ways of recovery: Compliance with the sanitary and hygienic regime (wet cleaning of premises at least 2 times a day, ventilation, hygienic baths, boiling and ironing of linen, proper storage of baby care items, proper treatment of the skin and umbilical wound ). Rational feeding, prevention of constipation and intestinal dysfunction. In the absence of risk factors up to 4 months and illnesses, the child can be transferred to the first health group. Risk group 3. For anemia Frequency of examinations by specialists: Pediatrician in the first year monthly. Particular attention is paid to: General condition, lethargy, loss of appetite, proper feeding, pallor of the skin, mucous membranes, condition of the gastrointestinal tract, hemogram indicators (hemoglobin not lower than 200 g/l in children 1-2 months old and 110 g/l in children -12 months). Additional research methods: Blood test for full-term infants once every 3 months, and monthly for premature infants. Risk group 3. For anemia. Main ways to improve your health: Balanced nutrition, avoiding overfeeding with dairy and flour products. Introduction of vegetable puree from 4 months, fruit juices rich in vit. C, egg yolk, homogenized puree with meat or liver - from 5 months. Preventive doses of iron supplements - 2-4 mg/kg of elemental iron per day from 3 months of age until the introduction of meat products into the diet. Particular attention is paid to sufficient time in the fresh air, massage, and gymnastics. In the absence of anemia, normal neuropsychic and physical development, and the absence of other risk factors, children by the age of 1 year can be transferred to 1 group. health. Risk group 4-5. For chronic nutritional disorders (hypotrophy, paratrophy) Frequency of examinations by specialists: Pediatrician 1 time per month. Children of the PB health group from 1 to 3-6 months. are examined once every 2 weeks, then once a month. Neuropathologist - at 1, 6, 12 months. Dr. specialists within decreed deadlines. Endocrinologist according to indications. Particular attention is paid to: Appetite, the presence of regurgitation and vomiting, emotional tone. The dynamics of physical development, the condition of the skin, its elasticity, tissue turgor, the severity of the subcutaneous fat layer, pastiness. Condition of the lymph nodes and thymus gland, central nervous system, body temperature, appearance of foci of infection. Additional research methods: Anthropometry monthly, general blood test once every 3 months. General urine analysis at 3 and 12 months, coprogram. According to the indications, feces for micro-landscape, trypsin activity, test with Dexylose, determination of sodium in sweat (test with pilocarpine). If you have a family history of diabetes, blood sugar is measured once every 3 months. (can be alternated with determination in urine). Risk group 4-5. For chronic nutritional disorders (hypotrophy, paratrophy) The main ways of recovery: Elimination of the causes contributing to the development of chronic nutritional disorders. Rational feeding. Tempering procedures, massage, gymnastics, sufficient exposure to fresh air, rational child care. Providing the family with scales. Risk group 6. For rickets Frequency of examinations by specialists: Examinations by a pediatrician and specialist doctors within prescribed periods. According to indications, orthopedic surgeon, nephrologist Particular attention is paid to: The condition of the musculoskeletal system: the size of the large and small fontanelles, the condition of their edges: the presence of softening and deformation of the bones of the skull, chest, ribs, limbs; muscle tone; timing and nature of teething; development of motor skills and abilities; the state of the neurovegetative sphere and internal organs and systems: cardiovascular, abdominal organs (liver, spleen). Additional research methods: Sulkovich reaction 1 time per month. Risk group 6. For rickets Main ways of recovery: Balanced nutrition of a nursing woman and child, maintaining natural feeding. When artificial feeding - use adapted mixtures; stay in the fresh air in the summer for 8-10 hours a day, in the winter - at least 3-4 hours; massage for a child from 1.5 months, gymnastics in combination with massage from 2.5-3 months; prevention of infectious diseases (acute and chronic). Specific prevention of rickets vit. D is carried out for full-term children from 3 weeks of age daily during the autumn-winter-spring periods of the year in the 1st and 2nd year of life at a dose of 1000 IU. A course of vitamin D is allowed (3 courses) during the 2nd, 6th, and 10th months of life; in the 2nd year of life, in the winter and spring periods of the year, 2 courses (30 days each) with an interval between them of no more than 3 months. The dose of vitamin D for 1 course ranges from 60,000 to 120,000 IU, the daily dose of vitamin D ranges from 2000 to 4000 IU. For premature babies, depending on the gestation period and the establishment of enteral nutrition, Vit D is prescribed from 10-20 days of life daily for the first 2 years, excluding the summer months, at a dose of 400-500-1000 and 1000-2000 IU. If there are no signs of rickets in the first year of life, a child at the age of 1 year is transferred to group I. health. Risk group 7. For the formation of malformations of the tissues of temporary and permanent teeth, caries and malocclusion Frequency of examinations by specialists: Pediatrician in the first year of life monthly, according to indications - dentist, orthodontist Particular attention is paid to: Timing and order of teething, change of teeth, condition surfaces of erupted teeth (presence of plaque), sucking activity, the appearance of bad habits (sucking fingers, lips, tongue), breastfeeding and bottle feeding techniques, posture and position of the child’s head during sleep, lip closure. Additional research methods: According to indications, x-ray of the jaws and anus. blood for calcium and phosphorus levels. The main ways to improve your health: A balanced diet, eliminating sweetened drinks and limiting the intake of sweet foods. Hygienic oral care. Compliance with feeding techniques, elimination of bad habits; when the lower jaw protrudes above the upper jaw, a low headboard is indicated; if, on the contrary, a high headboard is indicated. Ensure that the child's lips are closed while awake and asleep. Cleaning the surface of erupted teeth from plaque, applying to them for 2 minutes. gauze strips soaked in 10% calcium gluconate solution (remineralizing therapy) for 10-15 days every 3-4 months. In the first 6-8 months. after birth, with a reduced fluoride content in drinking water (below 0.8-1.0 mg/l), Vitaftor is prescribed 1 drop/kg for 5-6 months. Risk group 7. For the formation of malformations of the tissues of temporary and permanent teeth, caries and malocclusion Frequency of examinations by specialists: Pediatrician in the first year of life monthly, according to indications - dentist, orthodontist Particular attention is paid to: Timing and order of teething, change of teeth, condition surfaces of erupted teeth (presence of plaque), sucking activity, the appearance of bad habits (sucking fingers, lips, tongue), breastfeeding and bottle feeding techniques, posture and position of the child’s head during sleep, lip closure. Additional research methods: According to indications, x-ray of the jaws and anus. blood for calcium, phosphorus content Risk group 7. For the formation of malformations of the tissues of temporary and permanent teeth, caries and malocclusions. Main ways of recovery: Balanced diet, exclusion of sweetened drinks and limiting the intake of sweet foods. Hygienic oral care. Compliance with feeding techniques, elimination of bad habits; when the lower jaw protrudes above the upper jaw, a low headboard is indicated; if, on the contrary, a high headboard is indicated. Ensure that the child's lips are closed while awake and asleep. Cleaning the surface of erupted teeth from plaque, applying to them for 2 minutes. gauze strips soaked in 10% calcium gluconate solution (remineralizing therapy) for 10-15 days every 3-4 months. In the first 6-8 months. after birth, with a reduced fluoride content in drinking water (below 0.8-1.0 mg/l), Vitaftor is prescribed 1 drop/kg for 5-6 months. Risk group 8. For thymus enlargement syndrome Frequency of examinations by specialists: Pediatrician monthly in the 1st year of life and quarterly in the 2nd year. According to indications, consultation with an endocrinologist, neurologist, immunologist, ENT doctor. At the initial detection of thymomegaly - an endocrinologist, immunologist and ENT specialist at 2, 3 years. Particular attention is paid to: General condition, physical development, condition of the lymph nodes, tonsils, spleen, the presence of adenoids, the size of the vascular bundle in the 23rd intercostal space, signs of compression of the mediastinal organs (cough, oral cyanosis, swelling of the jugular veins, vascular network on the chest, hoarseness voices, persistent regurgitation, vomiting), symptoms of adrenal insufficiency (pigmentation and depigmentation, dark skin tone, muscle hypotension, general asthenia, decreased blood pressure, increased craving for salty foods), the presence of allergic reactions to vaccinations, prolonged low-grade fever. Additional research methods: According to indications - X-ray or ultrasound examination; if an enlarged thymus is detected, X-ray or ultrasound control is performed every 3-6 months, then annually until the thymus is normalized. Blood test at 3, 9, 12 months. According to indications, T and B lymphocytes, immunoglobulins, study of hormonal parameters as prescribed by an endocrinologist. Risk group 8. For the syndrome of enlarged thymus gland. Main ways of recovery: Rational regimen, hardening. Optimal nutrition, moderate consumption of fats and carbohydrates. Sanitation of chronic foci of infection, hyposensitizing and immunomodulatory therapy if indicated. For severe illnesses and stressful situations (surgeries) - corticosteroid replacement therapy. In the event of acute infectious diseases, hospitalization is recommended; less often, a home hospital with daily monitoring is organized. Deregistration after normalization of the size of the thymus. Risk group 9. For sudden death syndrome (SDS) Frequency of examinations by specialists: Pediatrician for the first 7 days daily, at 14, 21 days and at 1 month, then 2 times a month until 8 months. Subsequently - once a month. Neurologist and cardiologist at 1, 3, 6, 9, 12 months; immunologist and endocrinologist in the first 3 months, and then according to indications. Particular attention is paid to: Conditions for caring for the child in the family, the attitude of relatives towards him, the presence of clinical signs of immaturity, thymomegaly, adrenal insufficiency, dysfunction of the thyroid and parathyroid glands, attacks of cyanosis, apnea, loss of consciousness, vomiting and regurgitation syndrome, autonomic dysfunction, unmotivated attacks of anxiety and agitation, sinus bradycardia, tachycardia, arrhythmia, disturbances in repolarization processes, prolongation of the QT interval. Additional research methods: Determination of the risk group for VNS syndrome (according to the screening table) during primary care of a newborn. General an. blood and urine at 1,3 and 12 months. Neurosonography and ECG in the first 3 months. life. According to indications, cardiointervalography, Holter monitoring, Echo-CG, determination of vegetative status. Ultrasound of the thymus in the first 3 months. According to ultrasound indications - other endocrine glands. According to indications, computed tomography, nuclear magnetic resonance, study of blood electrolytes, immunological status, hormonal profile. Risk group 10. Children with manifestations of exudative-catarrhal diathesis. Frequency of examinations by specialists: Pediatrician once a month. More often during periods of active immunization. According to indications - allergist, dermatologist. Other specialists - within decreed terms. Particular attention is paid to: History (allergic diseases in the family, abuse of food allergens in the last 3 months of pregnancy, taking medications, severe toxicosis, prematurity and immaturity of the child, early artificial feeding, repeated courses of antibacterial therapy); condition of the skin and mucous membranes, tissue turgor, blood tests (leukopenia, eosinophilia, lymphocytosis), urine (proteinuria, microhematuria), feces (dysbacteriosis), coprogram (impaired digestion of food). Additional research methods: Blood and urine analysis once a quarter. According to indications, stool tests for micro-landscape and coprogram. Risk group 10. Children with manifestations of exudative-catarrhal diathesis. The main ways of recovery: Antigen sparing regimen. Exclusion of obligate food allergens from the diet of a nursing mother. The struggle for breastfeeding. When artificial feeding, the introduction of fermented milk or low-lactose mixtures. Use only freshly prepared juices (apple, cabbage, plum) for the purpose of fortification. Herbal medicine (decoctions of string, yarrow, mint, viburnum, birch leaf, licorice root, etc.). In the presence of dysbacteriosis, biological products (bifidum-bacterin, lacto-bacterin; from 6 months of age, bifikol, colibacterin). Combating intestinal dysfunction (constipation, impaired intestinal absorption). Active immunization is carried out with conventional types of vaccines at prescribed times with the prescription of antihistamines 2-3 days before and 3-5 days after vaccination. In addition, 7 days before and 7 days after, ascorutin, glutamic acid, and vitamin E are prescribed. Risk group 11. Children with manifestations of lymphatic-hypoplastic diathesis Frequency of examinations by specialists: The frequency of observation by a pediatrician is individual. For severe manifestations of diathesis, follow-up with an endocrinologist and immunologist 2 times a year in the first 3 years of life, then once a year. Other specialists - at designated times and according to indications. Particular attention is paid to: History (excessive nutrition of the pregnant woman, bacterial diseases during pregnancy, the presence of bronchial asthma, adenoiditis, chronic tonsillitis, chronic sinusitis, diabetes mellitus, obesity in the parents); large body weight at birth, physical development, motor and emotional activity, signs of hypocortisolism (lethargy in the afternoon, hypothermia, beads of sweat on the forehead, etc.), the child’s reaction to acute diseases, manifestations of lymphoproliferative syndrome Additional research methods: By indications - immunogram, study of renal excretion of 17 ACS, if thymomegaly is suspected, chest x-ray; ECG - 2 times a year. Clinical blood and urine analysis once a quarter. According to indications - blood sugar (if there is a family history of diabetes mellitus) once every 3 months. The main ways of recovery: Age-appropriate regimen with the exception of strong mental and physical irritants. Individual care up to 3 years of age. Natural feeding in the first year of life. When artificial feeding, fermented milk mixtures are prescribed. With prolonged intestinal dysfunction, limit fats to 4-5 g/kg body weight. In the future, a diet with a restriction of easily digestible carbohydrates and fats. Some limitation of obligate allergens is shown. Nutrition for children over 3 years old - according to age. Salt is not limited if the child feels the need for salty food. Drug therapy for children with thymomegaly is prescribed in courses 2 times a year - in spring and autumn: 1) short courses of desensitizing agents and herbs (chamomile, yarrow, birch buds and inflorescences, wild garlic, blueberries, sea buckthorn oil, etc. 2) gentle immunostimulation for 2 -x weeks (pentoxyl, eleutherococcus) 3) vitamins A; B1,2,5,15;P;C. 4) stimulation of the functions of the adrenal cortex (currant leaves, licorice root preparations) for 1-1.5 weeks. Adaptogens (ginseng tincture, pantocrine, golden root, zamanika, leuzea) for severe arterial hypotension. Pasty children - thyroxine. For severe bradycardia, regurgitation, and vomiting, anticholinergics are prescribed. If there are symptoms of compression of vital organs by the thymus gland, prednisolone is prescribed for 7-10 days. With the development of acute thymus-adrenal insufficiency - emergency care according to general principles. Gentle hardening methods according to an individual plan. Patient treatment of lymphoid tissue hyperplasia, adenotomy and tonsillectomy according to very strict indications. The issue of vaccination is decided strictly individually under the guise of desensitizing drugs. If there are signs of thymus-adrenal insufficiency, the terms of prof. Vaccinations are being postponed. Risk group 12. Children with manifestations of neuro-arthritic diathesis. Frequency of examinations by specialists: The frequency of observation by a pediatrician is individual. Observation by a neurologist and endocrinologist is indicated. Other specialists - at specified times and according to indications. Particular attention is paid to: Anamnesis (complicated heredity for disorders of salt metabolism, gastroenterological pathology, endocrine diseases, migraines), increased consumption by a pregnant woman (especially in the last trimester) of foods rich in purine bases, oxalic and ascorbic acids, caffeine, fats; signs of increased nervous excitability, the nature of mental development, symptoms of sensitive accentuation of character, intelligence, the presence of vomiting, vegetative neurosis, arthritis, allergoid reactions (Quincke's edema, urticaria, asthmatic syndrome, allergic dermatosis, etc.), a tendency to pain symptoms (renal, intestinal colic) . Additional research methods: Concentration of uric acid in blood serum, urine analysis at least once every 6 months. According to indications - urine for acetone. The main ways of recovery: The regime is protective, do not get carried away by the inquisitiveness and speed of mental reactions in these children, develop inhibitory reactions in them. Diet therapy is predominantly dairy-vegetable, enriched with potassium salts, an increased amount of liquid (rose hip decoction, syrups with cranberry, lingonberry jam, sea buckthorn juice, apple juice). Limitation of purine bases and some limitation of protein. Veal, poultry, and offal are excluded or limited; meat - boiled. Sausages, mushrooms, broths, jelly, some vegetables (sorrel, spinach, rhubarb, cauliflower, cabbage), yeast, oatmeal, polished rice, sauce, legumes, coffee, cocoa, strong tea, spices are eliminated. Diet therapy during acetonemic crises - fasting days - apple, watermelon, potato, etc. - 1-2 times a week. In case of acetonemic vomiting, a fasting pause for 10-12 hours, liquid by mouth or parenterally (physical, Ringer's solution, 5% glucose solution). Inside - sodium lactic acid. Correction of urine pH to prevent urolithiasis. For an acidic reaction - vit. B1 and B6, alkaline mineral waters, citrate mixtures blemaren, magurlit, solimak, urolit-5, etc. If the urine is acidic below 5.7, pepsin is prescribed 3 times a day for 10 days. Gymnastics, water procedures (baths, rubbing with warm, then cold water, showers) are shown. Herbal medicine (valerian root, motherwort herb, passionflower herb or combined preparations - passit and velosedan). If neurotic reactions intensify, tranquilizers (sibazon, diazepam, relanium, seduxen) are used. The course is 10-14 days. Active immunization is carried out within the prescribed time frame. Risk group 13. Children from socially disadvantaged families Frequency of examinations by specialists: Pediatrician the first 7 days after discharge from the maternity hospital - at 14, 21 days and 1 month. From 1 to 6 months - once every two weeks, from 6 to 12 months - once a month. According to indications - more often. Specialists - depending on the leading risk factors (ophthalmologist, speech therapist, psychoneurologist, geneticist, physical therapy doctor). Particular attention is paid to: History. General state. Proper feeding and care of the child. Dynamics of height, weight, head size, psychomotor development. The presence of congenital diseases, developmental anomalies, stigmas of disembryogenesis. Features of behavior and sleep. Availability of necessary accessories and toys for the child. The main ways of improvement: Joint work of the local pediatrician, legal advisers, commissions for the protection of motherhood and childhood and commissions for minors, public education authorities, internal affairs, social security, administration and public organizations at the place of study or work of parents, aimed at improving the health of life and relationships in family.
Premature baby: A premature baby is characterized by a disproportion of individual parts of the body: a relatively large head and torso in relation to height, a short neck and legs, a low navel. The brain skull predominates over the facial skull. The fontanelles (anterior, posterior, often mamillary and sphenoid) are open, the cranial sutures diverge. The bones of the skull are soft, pliable, and move one on top of the other. The ears are underdeveloped and soft. The nasal cartilages are also underdeveloped.
Diagnostic signs of prematurity: body weight from 1000 g to 2500 g, height cm, head circumference – cm, chest circumference – cm; functional and morphological immaturity of the main organ systems; decreased lecithin/sphingomyelin ratio in amniotic fluid, bronchial and gastric aspirates; external signs of immaturity (thin skin, underdeveloped ear cartilage, etc.); high levels (fetoprotein; late start of maturation of protective morpho-functional structures); high frequency of edema syndrome in the first days of life (40%), SDR (60-70%), intracranial hemorrhages, prolonged conjugative hyperbilirubinemia.

Features of the subcutaneous fat layer: There is no subcutaneous fat layer. The skin is thin, wrinkled, bright or dark red, sometimes glossy, shiny; covered with down (lanugo) on the forehead, cheeks, shoulders, back, and thighs. Because the skin is thin, the network of saphenous veins is visible, and the movement of the intestines can be seen through the abdominal wall. Cheese-like lubricant covers not only areas of physiological folds, but also the entire surface of the body. The nails on the fingers of the extremities are poorly developed and do not extend beyond the edge of the nail bed.

Premature baby: In girls, due to insufficient development of the labia majora, the genital slit is gaping, the clitoris is clearly visible, in boys the scrotum is bright red, empty, the testicles are contained in the inguinal canals or even in the abdominal cavity. The child is sleepy, muffled, and has a weak cry. Movements are uncoordinated and chaotic. Muscle tone is reduced. Physiological reflexes are weakened. Very premature babies may lack swallowing and sucking reflexes.

Activities to provide medical care to premature babies: 1. Hospitalization of women with premature birth in specialized maternity homes. 2. Application of careful delivery methods. 3. Creating optimal conditions for caring for a premature baby in the maternity hospital (stage I). 4. Creation of optimal conditions for nursing healthy premature babies (stage II) and treatment of sick premature babies. 5. Clinical observation of premature babies in a children's clinic.

Features of caring for a premature baby: In the delivery room, a woman with premature birth requires careful care. Childbirth is usually carried out naturally, carefully, without protection of the perineum, always by an obstetrician and neonatologist. Particular attention should be paid to the prevention, timely diagnosis and treatment of intrauterine hypoxia, as well as to prevent the child from cooling down. The temperature in the delivery room should be 2224 °C. It is imperative to prevent asphyxia for Nikolaev. The fetal heartbeat in the first period is listened to every 15 minutes, in the second period every 5 minutes.

Caring for a premature baby: Children who were born with asphyxia undergo a complex of resuscitation measures (suction of mucus, mechanical ventilation, chest compressions, injection into the umbilical cord vein of a 20% glucose solution, 10% calcium chloride solution, cocarboxylase, etimizol, ATP, analeptic mixture, prednisolone). Manipulations related to the revival of a premature baby, ligation of the umbilical cord, prevention of gonoblenorrhea, primary toileting, are carried out with mandatory additional heating with a heat lamp, on a heated changing table. The diapers and midwife's hands should also be warm. After spontaneous breathing is restored, the child is immediately transferred to the neonatal department.

Wards for premature babies: In the wards of the maternity hospital for nursing premature babies (stage I), the temperature should be 2326 °C. Functionally immature children, whose weight is less than 1800 g, are placed in a closed incubator such as “Inka”, “Medicor”, where it is possible to maintain the required temperature, humidity (6570%) and, if necessary, use oxygen. Children whose birth weight is less than 1200 g are kept in an incubator, the temperature in which during the first week becomes 36 °C, from the 7th to the 12th day 35 °C, from the 12th to the 15th day 34 °C, from the 15th to the 20th day 33 °C, after the 20th day 32 °C. For children whose weight reaches 1 g, the temperature should accordingly be 35°, 34, 33, 32 °C; for children whose weight is more than 1500 g, the temperature from the first days should not exceed °C. The duration of a premature baby's stay in the incubator depends on its ability to adapt to environmental conditions and is indicated by its ability to maintain a constant body temperature. On average, children who weigh more than 1200 g stay in the incubator for 314 days, and those weighing less than 1200 g from 14 to 30 days. Children weighing more than a gram are kept in open incubators with additional heating with heating pads (water temperature in the heating pads is 5060 °C) for the first 56 days.


Caring for premature babies: Manipulation, swaddling, examination of premature babies in the ward should be carried out with mandatory additional heating and strict adherence to the rules of asepsis and antiseptics. Much attention is paid to the prevention of attacks of secondary asphyxia and respiratory distress syndrome. A significant role is played by the correct gentle swaddling of the child, ensuring maximum rest, the appointment of mustard plasters on the chest 23 times a day, the use of oxygen at 4050% concentration, etimizol, inhalation with substances that stabilize the surfactant (glycerin 1 ml, heparin 50 units/kg body weight, isotonic sodium chloride solution 3 ml) 3 4 times throughout the day. If premature babies are diagnosed with a disease, they are treated at the first stage and in specialized departments.

Stage II of nursing for premature babies: Children whose weight on the 7-10th day of life is less than 2000 are transferred to Stage II of nursing. The main tasks of this stage are: 1) creating optimal environmental conditions; 2) rational nutrition; 3) prevention of rickets and anemia; 4) massage, exercise therapy; 5) treatment of various pathological conditions.

Care for premature babies: Particular attention is paid to the sanitary and hygienic regime and care for premature babies. The temperature in the rooms is 2425 °C, they do wet cleaning and ventilation. Premature babies are bathed in boiled water (temperature 3840 °C) for 5 minutes. After the bath, the child is wiped with a dry diaper, swaddled in warm, clean linen, and swaddled again after a minute. Very premature babies stay in incubators until they independently maintain a constant body temperature. To warm children in regular wards, heating pads are used; the water temperature in them should not exceed 60 °C. One heating pad is placed under the blanket on the legs and two heating pads are placed along the child’s body on both sides on top of the blanket.

Prevention of rickets and anemia in premature infants: To prevent rickets, from the 810th day of life, ergocalciferol (vitamin D) in an oil or alcohol solution is prescribed, IU per day for 25 days (per course of IU) and calcium supplements. Instead of using ergocalciferol, ultraviolet radiation can be performed (25 sessions). To prevent anemia, it is advisable to introduce microelements into the child’s diet from three weeks of age. Midi sulfate (0.01% solution, 1 ml/kg body weight) and cobalt sulfate (0.001% solution, 0.2 ml/kg body weight) are added to breast milk or formula once a day for 610 weeks. Iron supplements (hemostimulin, iron lactate, etc.) are prescribed from eight weeks of age for 35 months.

Nursing premature babies: When nursing premature babies, one should consider their characteristic deficiency of iron and vitamins. From the first days of life, they need to be prescribed retinol, tocopherol, thiamine, riboflavin, pyridoxine, rutin, ascorbic and nicotinic acids. Premature babies are discharged home when they have reached body weight g and are in satisfactory general condition.

Caring for premature babies in the area: Monitoring of premature babies in the area should be carried out by a local pediatrician with the help of a visiting nurse. Children whose birth weight is below 1700 g are visited by a nurse 4 times a month by the age of 7 months, children with a body weight of more than 1700 g twice a month by 4 months, and then once a month.

Basic principles of clinical examination of premature infants: 1) dynamic monitoring of physical and psychomotor development; 2) control over rational feeding; 3) prevention, early diagnosis and treatment of rickets, anemia; 4) timely detection and treatment of neurological and orthopedic disorders.

Nutrition of premature infants: Nutrition of premature infants depends on age, body weight at birth, degree of maturity, and general condition. The first feeding of healthy premature babies is prescribed after an hour; for children with manifestations of respiratory distress syndrome (RDS) 
Nutrition of premature infants: Feeding technique is indicated by the presence of sucking and swallowing reflexes and the general condition of the child. The weakest children need to be fed through a permanent factory-made polyethylene tube with a rounded smooth end or through rubber catheters 9 and 10. The polyethylene tube is inserted through the nasal passages, the rubber tube only through the mouth. When inserting the probe into the stomach, fix it above the upper lip and leave it on the face with an adhesive plaster for 4872 hours, pull it out, boil it and, if necessary, insert it again. Milk is introduced into the stomach in drops, after introducing the entire amount, the probe is washed with 12 ml of 10% glucose solution. This feeding method is used in the first or second week of life until the sucking reflex appears, after which they combine a one-time insertion of a tube with bottle feeding, gradually switching to bottle feeding, and then breastfeeding.

Feeding premature babies: Children with well-defined sucking and swallowing reflexes, whose body weight is less than 1700 g, should be bottle-fed. If the baby actively sucks, does not spit up and does not get tired when feeding, he can be applied to the breast 12 times a day with a gradual transition to breastfeeding.

Feeding premature babies: Healthy premature babies weighing more than 1700 g should be placed on the mother's breast as early as possible. Breastfeeding is carried out with mandatory control weighing. If the baby does not suck enough breast milk, then you need to supplement with breast milk from a bottle. It is most rational to feed a premature baby every 3 hours, initially 8 times a day (without a night break), and later 7 times a day (with a 6-hour night break). The daily amount of milk is best determined using this method: on the first day of feeding, children who weigh less than 1500 g should receive ml of milk; children whose weight is more than 1500 g ml. In the following days, the daily amount of milk for children whose body weight is less than 1500 g is increased every day by 1530 ml, and for children whose body weight is more than 1500 g per ml. On the 1st day of life, the amount of milk a child needs per day should be 1/5 of his body weight.

Feeding premature babies: Human milk is an ideal food for a premature baby, but it cannot replace the need for protein, and sometimes fat, in children born with a body weight of less than 2000. In these cases, nutrition is corrected with formula. If there is no breast milk, premature babies can be given adapted formulas (Nan, Nutrilon, Detolakt).

24
OBIECTIVELE lECŢIEI: O1 - Să caracterizeze perioada de nou –născut
O2 – Să definească noţiune de nou-nascut
prematur
O3 – Să numească gradele prematurităţii
O4 – Să enumere factorii de risc
O5 – Să numească semnele nou-născutului
prematur.
O6 – Să enumere criterii de externare
O7 – Să efectueze toaleta matinală, intimate, băiţa
In conditions of horizontal differentiation, the buyer's choice is determined by commitment to a particular brand,...
Vertical product differentiation involves the distribution of products in an industry market in accordance with their...

A citizen of the Russian Federation (each individual) is a consumer of state resources: water (for hot and cold), electricity, etc....
In many areas of life there are such concepts as centralization and decentralization. These concepts entered the written...

Get acquainted with draft orders of management relating to its activities. 3.8. Sign and endorse documents...

08/23/2019 Every citizen who has an official place of employment has the right to go to. But no one...

1. Working conditions according to the degree of harmfulness and (or) danger are divided into four classes - optimal,...

Decree of the Government of the Russian Federation dated April 30, 2013 N 382 (as amended on October 1, 2018) “On holding a public...

Corvette "Boikiy" (hull number 532) is the third in a series of Project 20380 ships built by JSC...
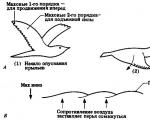
Let's consider the horizontal air flow relative to the inclined surface of the wing in the case when it...
1. Is the statement true: “Caring for offspring leads to a reduction in the birth rate in animals”? Prove your point...

Features and habitat of the burial ground bird It’s simply amazing why it wears such a proud, beautiful...

1. Definition and origin of life script. Script theory was first developed by Eric Berne and...

General information about the use of online cash registers In accordance with Federal Law No. 290-FZ dated 07/03/2016...
Vertical product differentiation involves the distribution of products in an industry market in accordance with...

A citizen of the Russian Federation (each individual) is a consumer of state resources: water (for hot and cold),...